
















Genetic scores are booming. But will anti-discrimination laws cover your DNA?
Imagine this scenario: During a routine visit, your doctor runs a new genetic test that shows you are at a tremendously increased risk of a future heart attack. You’re in shape; You feel good. But prediction is in your DNA.
The next day, you tell your employer that your doctor wants you to make some adjustments—switch to a less physically demanding job, or perhaps lower your stress levels to save your life. Can your boss legally deny you these accommodations? According to current law, yes.
That’s because federal regulations protecting employment and insurance discrimination based on genetics were not written with this technology in mind. While the Genetic Information Nondiscrimination Act of 2008 (GINA) protects employees from being fired because of their genetic test results and the Americans With Disabilities Act protects people with active disabilities, neither law compels an employer to make accommodations to reduce an individual’s future health risk.
This could become a problem as a new type of personalized medicine called polygenic risk scoring becomes increasingly popular. The technology uses DNA to estimate a person’s likelihood of developing a particular disease. Legal and health researchers fear that our legal framework is falling behind as genomic tools advance rapidly – which in some cases could lead to the outright dismissal of those who use genetic testing.
“These polygenic risk assessments are going to become an increasingly important part of your life,” said I. Glenn Cohen, a professor at Harvard Law School who specializes in the intersection of bioethics and law and co-authored a report on the topic. “For me it is a great opportunity to reopen questions about the rules – questions that are rightly difficult from a political perspective.”
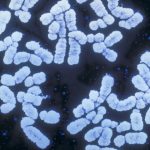
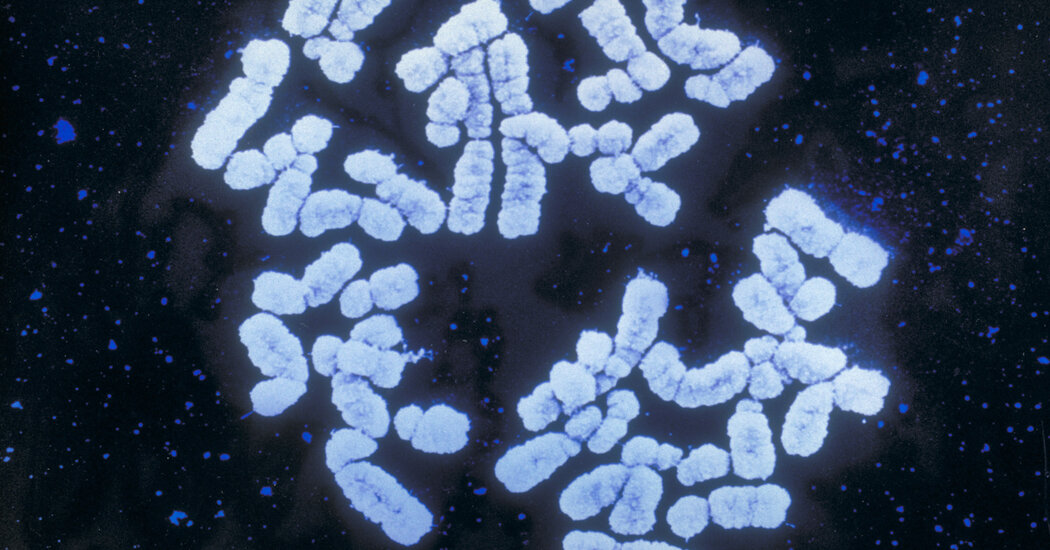
To understand the legal delay, it is helpful to first consider how the science of risk prediction has evolved. When many people think of genetic testing, they imagine monogenic tests that look for specific gene mutations that cause certain diseases, such as Huntington’s disease or cystic fibrosis. However, polygenic risk scores look for a range of variants throughout a person’s genome and combine the information into a cumulative estimate of their risk of developing a disease such as diabetes or cancer. If a monogenic test is like finding a cut wire that cuts off the sound of a speaker, a polygenic risk score is like a soundboard with dozens of switches that can combine to produce a dangerous frequency.
When GINA, the main law preventing genetic discrimination, took effect nearly two decades ago, companies were barely able to map individual genomes at an affordable price. GINA was written for the cut wire, not the soundboard.
Sam Trejo, a quantitative sociologist at Princeton University who studies polygenic risk scores, warned that GINA is “definitely not enough” to protect people from the situations they may face in the coming decades. “We need more robust protections there – we treat DNA like some kind of protected class,” he said.
Even among medical experts, there are still many unknowns when assessing polygenic risk. For example, a high risk score for heart disease does not mean a clear structural defect is identified, but rather a complex mix of genetic influences that could affect your taste buds and cravings, your propensity for exercise, or even a personality trait that attracted you to a job with high levels of stress, Dr. Trejo. Since the algorithms behind the ratings only draw correlations, the causes and effects of a rating remain unclear.
If the medical field doesn’t fully understand how to interpret polygenic scores, it makes sense that the workplace doesn’t either. Still, doctors agree that lifestyle changes can help balance certain genetic predispositions — which is why they might encourage patients with certain polygeny scores to minimize their risks in the workplace.
This is where the legal concerns lie. Researchers from Harvard Law School and Yale Law School who recently examined the regulatory gap uncovered an important gap in workplace accommodations. For example, a construction company cannot fire a healthy worker because of a polygenic test result for fear of future health care costs; However, the company may refuse the employee’s request for less strenuous work. That’s because GINA does not require employers to provide accommodations, and while the ADA does, that law does not consider genetics alone to be a disability subject to these rules.
In a recent case, Darby v. Childvine Inc., a plaintiff with a BRCA1 mutation linked to breast cancer was fired after she requested an exemption for a double mastectomy. The U.S. Court of Appeals for the Sixth Circuit ruled that “a genetic mutation that merely predisposes a person to other diseases, such as cancer, does not itself constitute a disability under the ADA.”
There is also a legal dead zone for employees who experience mild symptoms of illness, as GINA only protects those for whom the illness has not yet manifested itself, while the ADA requires accommodations only for those whose disabilities interfere with major life activities. So if supervisors at a chemical plant knew of a healthy worker with a high polygenic risk score for a rare lung disease, the employee could be fired immediately if he developed mild shortness of breath, the scientists said. GINA protections could disappear while standard ADA protections would not yet apply, leaving the employee to rely on difficult-to-prove legal exceptions to save the job.
In addition to workplace rules, GINA also prohibits health insurers from adjusting premiums or denying coverage based on genetic information. However, the law does not cover life, disability or long-term care insurance, which is why many people with genetic variants that are associated with a high risk of dementia are unable to obtain long-term care insurance.
Polygenic risk scores are still far from their full potential. The results do not provide medical certainty; They simply estimate a person’s risk of developing a particular condition relative to the population used to train the algorithm. Because they rely on the relatively small effects of many genetic variants, tests for some diseases require data from many more people to reduce statistical noise and improve their accuracy. Currently, some results may be misleading, particularly for people of non-European descent, who are underrepresented in many models.
Still, the test is growing in popularity: The direct-to-consumer market has grown, and at least one company has applied to the Food and Drug Administration for approval of its test to measure inherited genetic risk of coronary heart disease. Population geneticists and some doctors are advocating for wider use in clinics, saying the strongest algorithms could influence important decisions in patient care, such as when to start prescribing statins.
Some also say polygenic risk scores could be incorporated into so-called composite scores, integrating genetic data with other traditional measures such as diet, smoking status and body mass index, to increase their accuracy. But here too, legal scholars see an ambiguity, as factors such as age and gender are explicitly excluded in the GINA. Does GINA still apply if genetic data only makes up part of your score?
“I don’t want to give anyone the idea that this is a strong reason not to do it,” Cohen said. “My message is really to lawmakers: If you believe that these polygenic risk levels are good for public health, maybe you can close these gaps.”









{kind=link}